
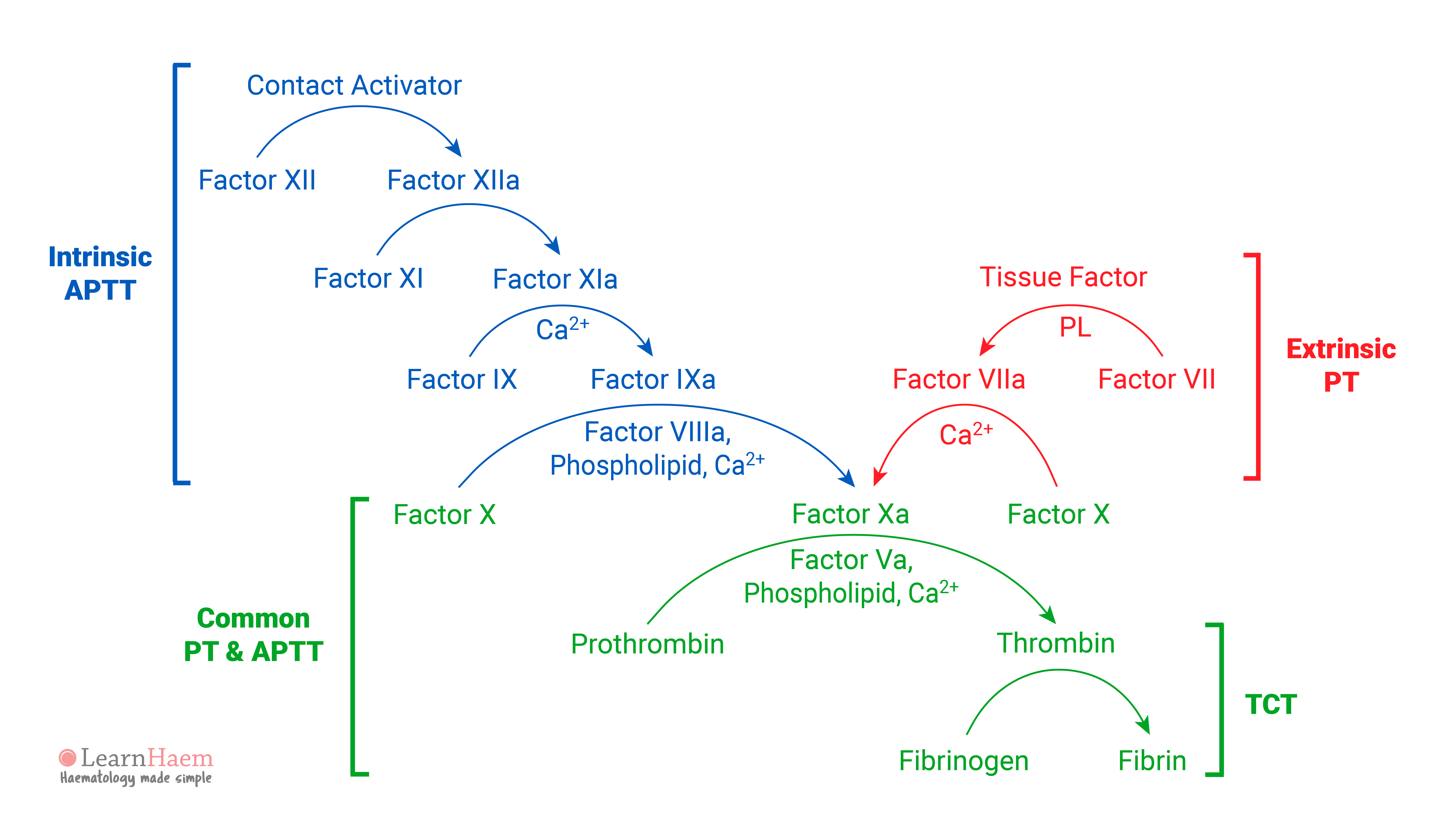
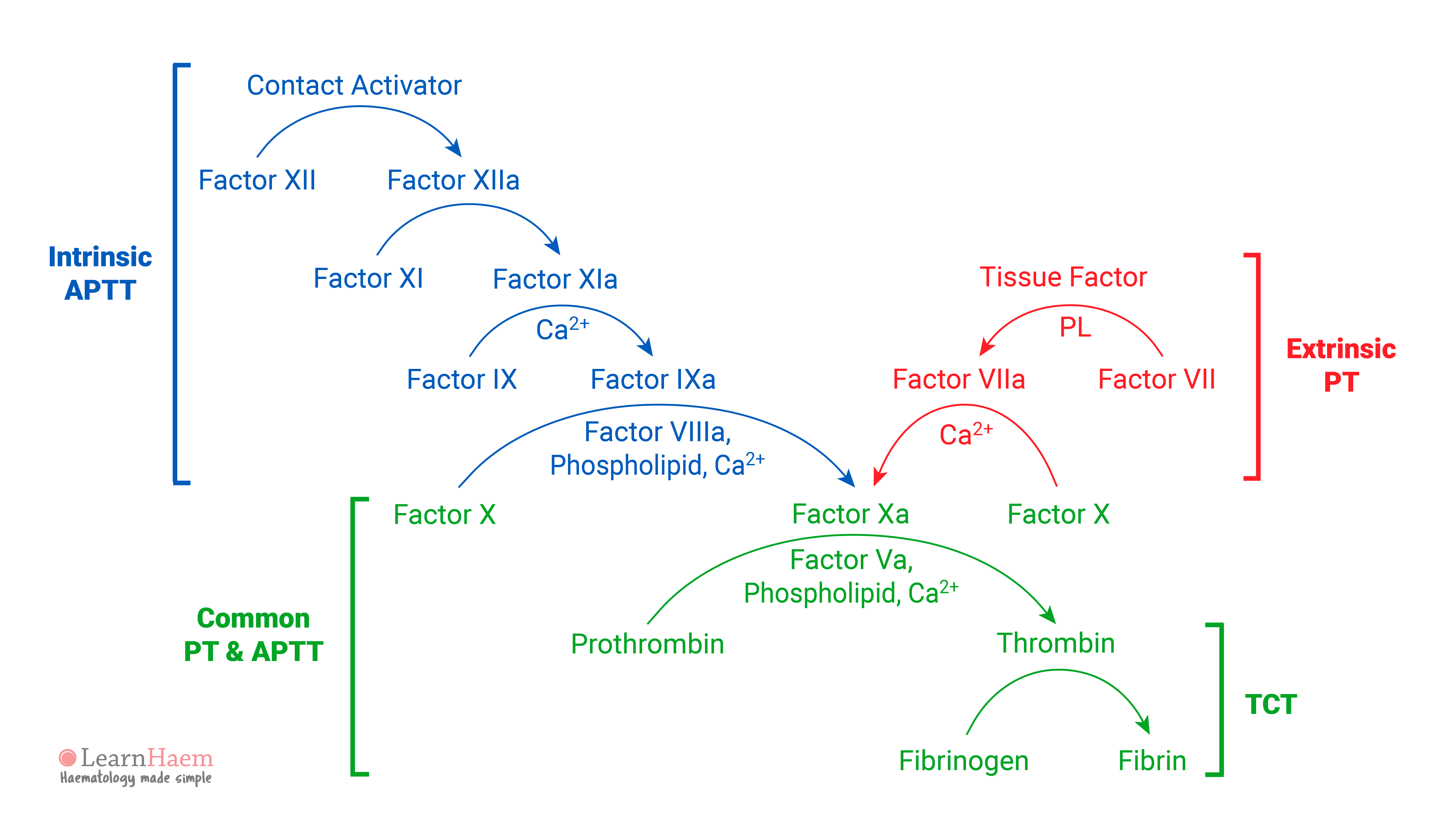
This depicts the intrinsic and extrinsic pathways of the revised model of the coagulation cascade. Although this is not how coagulation works in vivo (it cannot be, as it does not explain why haemophilia is a bleeding disorder, or why factor XII deficiency is not associated with a bleeding tendency), it is still useful to understand as it provides a framework for interpreting basic coagulation tests – the activated partial thromboplastin time (APTT), prothrombin time (PT) and thrombin clotting time (TCT).
- APTT: this is a reflection of the intrinsic pathway. Isolated prolongations of APTT should prompt considerations of factor VIII, IX, XI or XII deficiency. Of these, factor VIII (haemophilia A) and IX (haemophilia B) deficiencies can cause severe bleeding tendencies depending on the factor levels. Factor XI deficiency (haemophilia C) has a variable phenotype ranging from asymptomatic to severe bleeding. Factor XII deficiency is not associated with a bleeding disorder.
- PT: this is a reflection of the extrinsic pathway. Isolated prolongations of the PT are most often due to factor VII deficiency.
- Common pathway: deficiencies in factors V, X, thrombin and fibrinogen prolong both the APTT and the PT, as they are in the common pathway.
- TCT: this is a measure of the final step in the coagulation pathway, the conversion of fibrinogen to fibrin via the action of thrombin. It is hence sensitive to deficiencies in fibrinogen and drugs such as direct and indirect thrombin inhibitors.
Is it typing error for haemophilia C as it should be factor XI? correct me if i’m wrong
You are right. It is a typo. Thanks for highlighting!
Typo in the diagram – activated partial thromboplastin time is APTT, not APPT. This is correct in the text but not the diagram.
Thanks for highlighting this! You are correct 🙂
Does factor VIIa not also activate factor IX?