
There are two different variations in the Coombs test, but they both work on the same principle and are shown below. The direct Coombs test (DCT) is a test for the presence of pre-formed antibodies adherent to the red cell surface. In contrast, the indirect Coombs test is a test looking for the presence of specific antibodies in a patient’s plasma.
Although the Coombs test is often indicative of an immune-mediated process, it must be interpreted in the appropriate context. Ideally, it should only be sent in a haemolysing patient. False positives can be caused by certain medications (e.g. intravenous immune globulin), paraproteinaemia and recent transfusions.

The Direct Coombs Test. The DCT is a test which is done to look for pre-formed antibody adherent to the red cell surface. It is hence a test of immune-mediated haemolysis. A polyspecifc Coombs reagent, which binds to IgG, IgM or complement fragments. Normal individuals should have a negative DCT because they do not have antibodies on their red cells. Patients with immune-mediated haemolysis, such as autoimmune haemolytic anaemia, cold haemagglutinin disease, haemolytic transfusion reactions, haemolytic disease of the newborn, paroxysmal cold haemoglobinuria or certain types of drug-induced haemolysis will have a positive DCT.
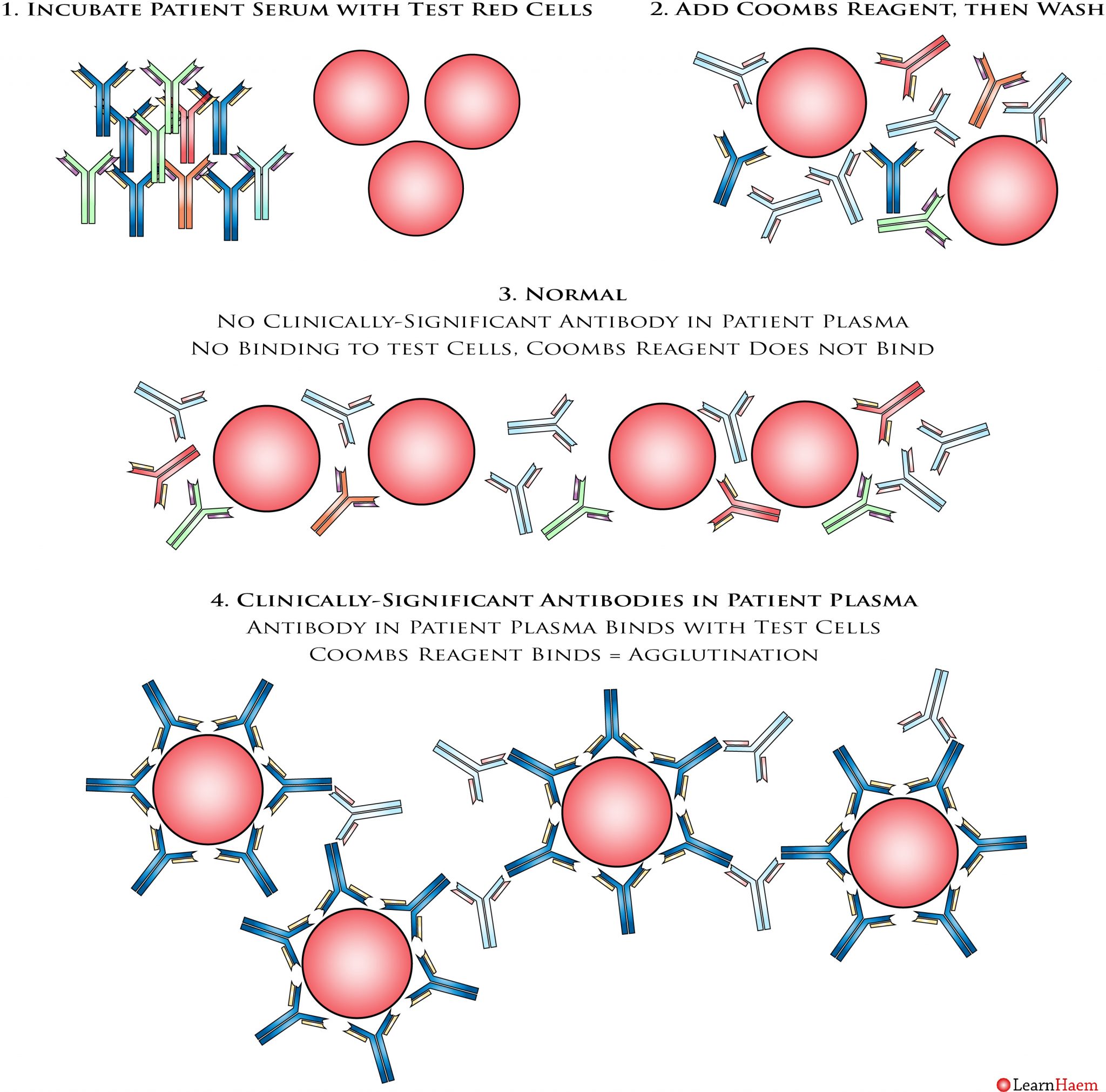
The Indrect Coombs Test. In contrast to the DCT, the indirect Coombs test aims to look for specific antibodies in the patient’s serum. The usual application for this test is in blood banking, to ensure that a patient does not have any clinically-significant alloantibodies, against certain red cell antigens, which may preclude routine transfusion. In order to do the test, the patient’s serum is incubated with a panel of red cells (test cells) which express a variety of known antigens. After this, the Coombs reagent is added. After allowing the reagents to incubate, the mixture is washed, which removes anything not bound to a red cell surface. In a normal situation, a patient should not have any clinically-significant red cell alloantibodies. Hence, there should be no reaction between the patient’s plasma and the test red cells. In a situation where there is a clinically-significant red cell antibody, the antibody in the patient’s plasma will bind to the test red cells. When the Coombs reagent is added, agglutination occurs, resulting in a positive indirect Coombs test.
Leave A Comment