
- Decompensated, acquired, immune-mediated haemolytic anaemia
- Incidence 1 in 100,000
- Classified serologically:
- Warm (65%)
- Cold haemagglutinin disease (29%)
- Paroxysmal cold haemoglobinuria (1%)
- Mixed AIHA (5%)
- 50% of cases are primary, 50% have an underlying cause.
- Drug-induced AIHA is also recognised, incidence ~1 in 1,000,000
- Clinical features:
- Warm AIHA: typically presents with symptomatic anaemia
- CHAD: may present with acrocyanosis, Raynaud phenomenon or symptoms of anaemia
- Polyspecific DCT (IgG and C3d) is usually positive in AIHA.
- Warm AIHA: IgG only (35%), IgG + C3 (56%), C3 only (9%)
- CHAD: usually C3 only, ~25% also have IgG
- PCH: C3 only
- Mixed AIHA: IgG and C3 (requires demonstration of warm and cold antibody with a high thermal amplitude >=30°C)
- Drug-induced AIHA: IgG, IgG+C3, C3 only or negative


0 x
0 x
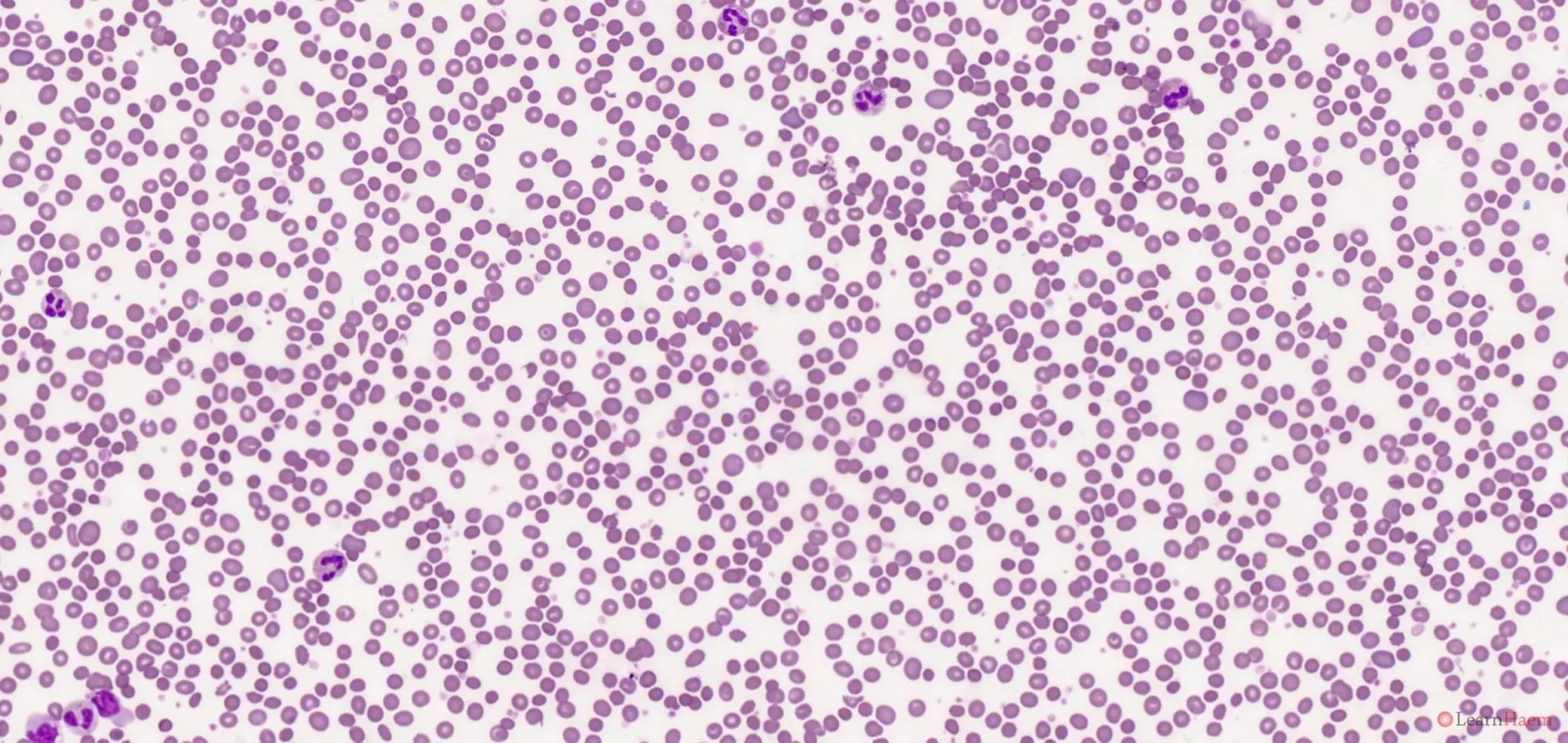
Blood film features:
- Spherocytosis
- Polychromasia with polychromatic macrocytes
0 x
This is the blood film of a patient who had a severe delayed haemolytic transfusion reaction.
Differential diagnosis:
- DCT Positive (IgG)
- Primary immune-mediated AIHA
- Haemolytic transfusion reaction
- ABO incompatible stem cell transplant
- Passenger lymphocyte syndrome
- +/- Drug-induced AIHA
- DCT Negative
- Hereditary spherocytosis
- Paroxysmal nocturnal haemoglobinuria
0 x
0 x
0 x
0 x
The four slides above show blood films and bone marrow aspirates from a patient who had AIHA secondary to B-prolymphocytic leukaemia.
Other features to look for / exclude:
- Atypical lymphoid cells
- Thrombocytopaenia (may have associated immune thrombocytopaenia)
- Agglutination
Causes:
- Primary immune-mediated warm AIHA
- Secondary
- Malignancy (especially chronic lymphocytic leukaemia)
- Infection (hepatitis C, tuberculosis, HIV etc.)
- Autoimmune disease
- Connective tissue disease (especially SLE)
- Inflammatory bowel disease
- Post-transplantation
Leave A Comment