
ß thalassaemia can interact with haemoglobin variants, such as haemoglobin E and haemoglobin S, to produce clinically-significant phenotypes which range in severity from transfusion-dependent anaemias to chronic moderate anaemias.
A high RBC count with a microcytic anaemia is typical of the ineffective erythropoiesis and shortened red cell survival in ß thalassaemia.
ß thalassaemia mutations are common in the Mediterranean, India, Southeast Asia. They can occasionally be seen in Afro-Caribbeans.
Haemoglobin E is a variant haemoglobin caused by a point mutation in the ß globin gene. It is common in Southeast Asia and the Indian subcontinent.
Patients with Hb E / ß thalassaemia usually have a thalassaemia intermedia phenotype, although some have a thalassaemia major phenotype, depending on the severity of the ß globin gene mutation.


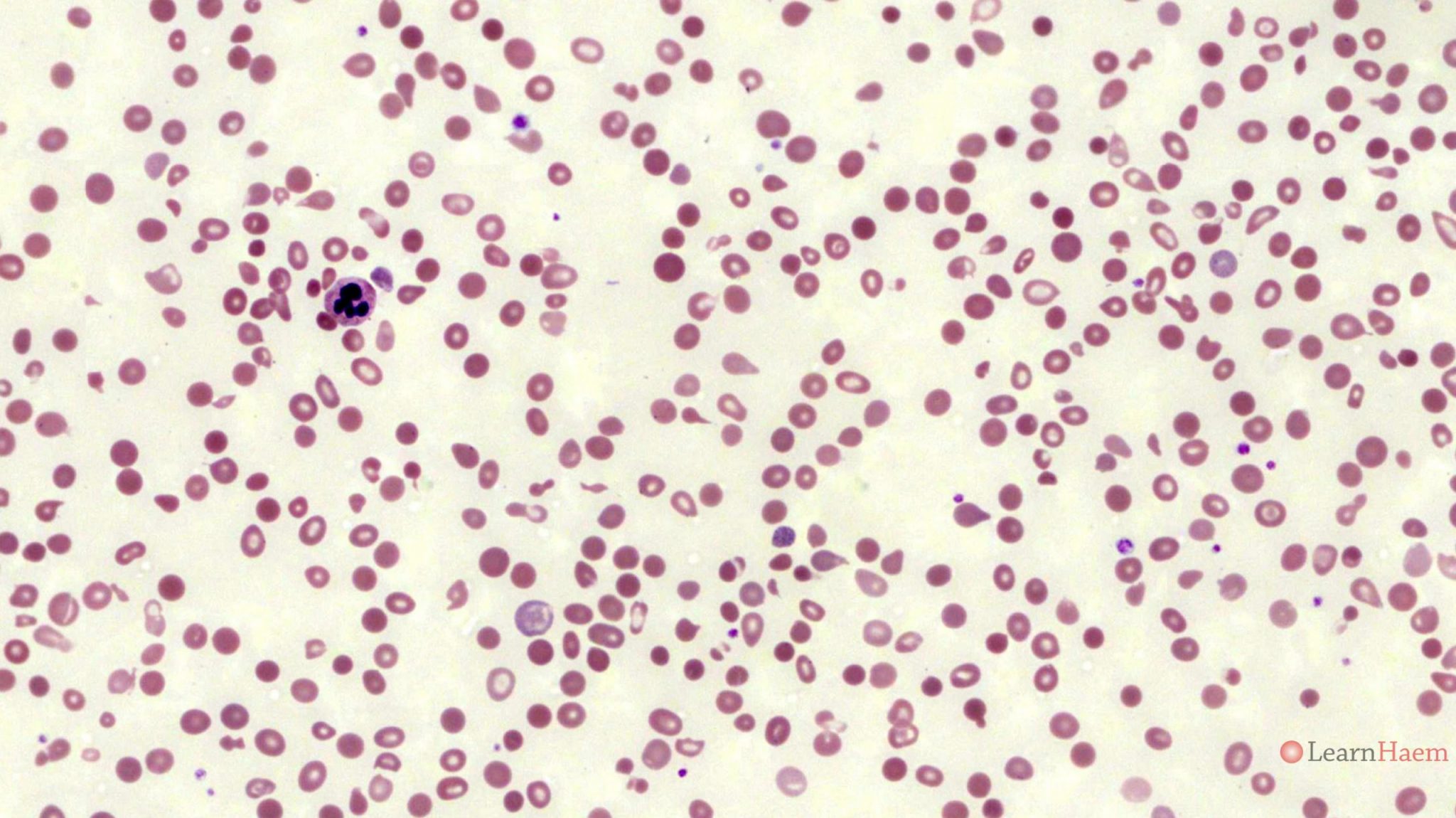
Blood film features:
- Moderate anaemia
- Marked anisopoikilocytosis
- Target cells
- Basophilic stippling
- Pappenheimer bodies
- nRBCs vary in quantity from occasional to very frequent (see another example of a blood film from a ß thalassaemia intermedia patient below)
Patient who has transfusion-dependent HbE/ß thalassaemia. This peripheral blood film was taken post-transfusion and some years after a splenectomy.
Other features to look out for:
- Splenectomy changes
- Dimorphic picture (transfusion-dependent patient with post-transfusion sample)
Haemoglobin electrophoresis:

Alkaline gel electrophoresis from a patient with HbE/ß thalassaemia (lane 8). There is no normal haemoglobin A. There are two bands, one with the mobility of haemoglobin F, and the other with the mobility of haemoglobin C. The differentials for a band with the mobility of haemoglobin C are haemoglobins C, E, O-Arab and A2.

Acid gel electrophoresis from a patient with HbE/ß thalassaemia (black arrow). There are two bands. The first has the mobility of haemoglobin F (red arrow). The second has the mobility of haemoglobin A (blue arrow). This excludes haemoglobin C and O-Arab as differentials for the band seen in the alkaline gel. The possibilities now are haemoglobin E or haemoglobin A2.
HPLC:

HPLC from a patient with HbE/ß thalassaemia. There is no normal haemoglobin A. 45% of the haemoglobin present is haemoglobin F (red arrow). 48% is in the A2 window (blue arrow). This fraction is too high for haemoglobin A2 alone, and represents a combination of haemoglobin E and haemoglobin A2.
The diagnosis is hence a compound heterozygote for haemoglobin E and ß0 thalassaemia (compound heterozygotes of haemoglobin E and ß+ thalassaemia would still have some normal haemoglobin A).
Other resources:
- PHE Family Origin Questionnaire
- PHE Sickle Cell and Thalassaemia Screening Programme (2019)
- BCSH Guideline: Significant Haemoglobinopathies: Guidelines for Screening and Diagnosis (2010)
- BCSH Guideline: Red blood cell specifications for patients with hemoglobinopathies: a systematic review and guideline (2020)
- RCOG Guideline: Management of ß Thalassaemia in Pregnancy (2014)
- TIF Guideline: Management of Transfusion Dependent Thalassaemia (2014)
- TIF Guideline: Management of Non-Transfusion Dependent Thalassaemia (2017)
Thank you . very interesting case studies.