
Microangiopathic haemolytic anaemia (MAHA) occurs when endothelial damage and / or fibrin deposition damages red cells, causing fragmentation. MAHA is a morphological finding which usually occurs in concert with a clinical thrombotic microangiopathy.


0 x
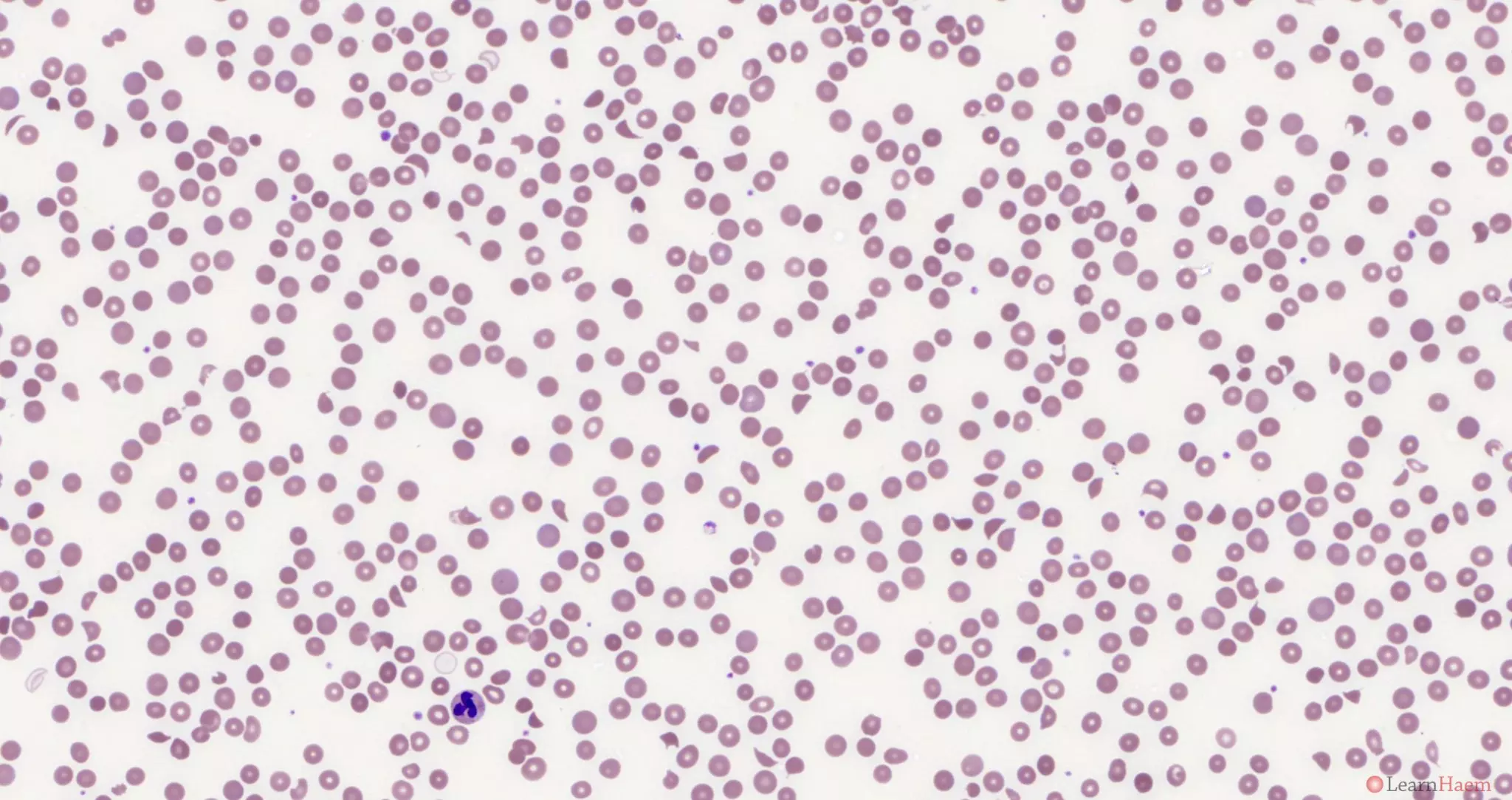
Blood film features:
- Schistocytes
- Microspherocytes
- Polychromasia with polychromatic macrocytes
- Thrombocytopaenia
Differential diagnosis
- Congenital
- Congenital ADAMSTS13 deficiency
- Congenital complement gene mutations
- Primary immune-mediated thrombotic microangiopathies
- Thrombotic thrombocytopaenic purpura (autoantibody against ADAMSTS13)
- Atypical haemolytic uraemic syndrome (autoantibody against complement factor H)
- Secondary thrombotic microangiopathies
- Pregnancy-associated (HELLP, pre-eclampsia)
- Malignant hypertension
- Malignancy-associated
- Transplant-associated
- Autoimmune-associated
- SLE
- Catastrophic antiphospholipid syndrome
- Glomerular disorders
- Disseminated intravascular coagulation
- Pancreatitis
- Drug-induced TMA (e.g. quinine, gemcitabine, bleomicin, penicillin, oxymorphone etc.)
- Mechanical haemolysis (e.g. cardiac valve haemolysis)
- Infection-associated
- Haemolytic uraemic syndrome (Shiga toxin producing E. coli)
- HIV-associated
Other resources:
- BCSH Guideline: Diagnosis and Management of TTP and other TMAs (2012)
- ISTH Draft Guideline: Diagnosis and Management of TTP (2019)
- ASH Image Bank: MAHA
- ASCO Post: MAHA Expert Review Case
- Syndromes of Thrombotic Microangiopathy (NEJM 2014)
- Transplant-Associated Thrombotic Microangiopathy (BMT 2017)
- Hereditary TTP (NEJM 2019)
Leave A Comment