
ß thalassaemia results from deletions in the ß globin gene. A normal human has 2 ß globin genes. Deletions in ß genes result in imbalanced synthesis of α globins and ß globins. As a result, excess free α globin chains accumulate and precipitate in red cell precursors, interfering with maturation and resulting in intramedullary destruction of erythroid precursors. This is known as ineffective erythropoiesis. The RBCs that enter the circulating contain varying amounts of free α globin (the amount increases with the phenotypic severity of the ß thalassaemia). The α globin and its breakdown products are deleterious to the red cell membrane, causing it to become more rigid and resulting in shortened red cell survival.
A high RBC count with a microcytic anaemia is typical of the ineffective erythropoiesis and shortened red cell survival in ß thalassaemia.
ß thalassaemia mutations are common in the Mediterranean, India, Southeast Asia. They can occasionally be seen in Afro-Caribbeans.
Patients with ß thalassaemia intermedia have a microcytic, hypochromic anaemia which is moderate which, by definition, does not require transfusion support. However, regular transfusions may be necessary to suppress extra-medullary haematopoiesis and its deleterious effects.


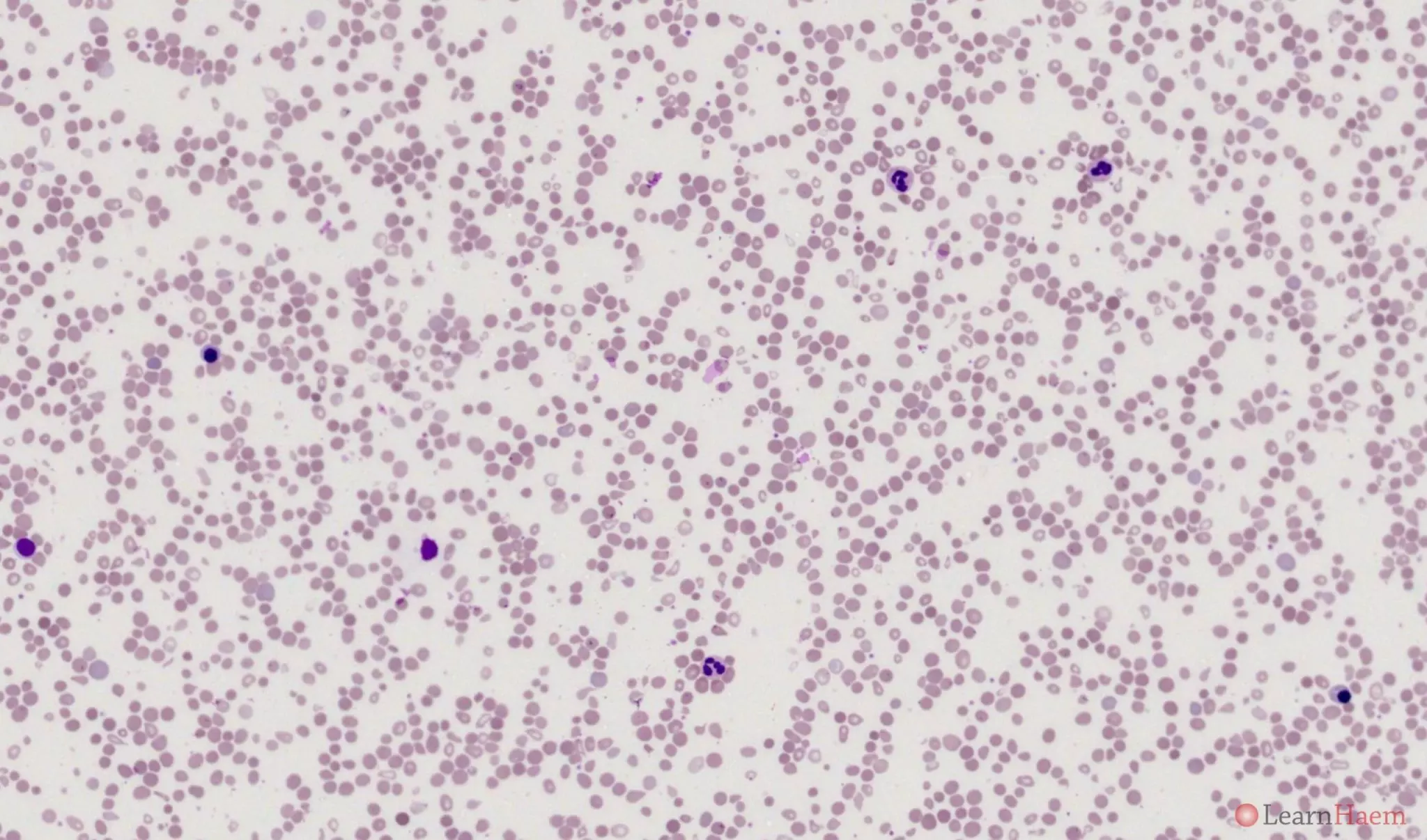
Blood film features:
- Moderate anaemia
- Marked anisopoikilocytosis
- Target cells
- Basophilic stippling
- Pappenheimer bodies
- nRBCs vary in quantity from occasional to very frequent (see another example of a blood film from a ß thalassaemia intermedia patient below)
Patient who has ß thalassaemia intermedia with marked extramedullary haematopoiesis. This blood film was taken post-transfusion. The patient also had a splenectomy in childhood.
Other features to look out for:
- Splenectomy changes
- Dimorphic picture (transfusion-dependent patient with post-transfusion sample)
Haemoglobin electrophoresis:

Alkaline gel electrophoresis from a patient with ß thalassaemia intermedia. There are three bands with the mobility of haemoglobin A (red arrow), haemoglobin F (green arrow) and haemoglobin C (blue arrow). The differentials for a band at Hb C are haemoglobins C, E, O-Arab and A2.

Acid gel electrophoresis from a patient with ß thalassaemia intermedia. There are two bands, one with the mobility of haemoglobin A (red arrow) and another with the mobility of haemoglobin F (green arrow). This excludes haemoglobin C and O-Arab as potential causes for the band at Hb C in the alkaline gel.
HPLC:
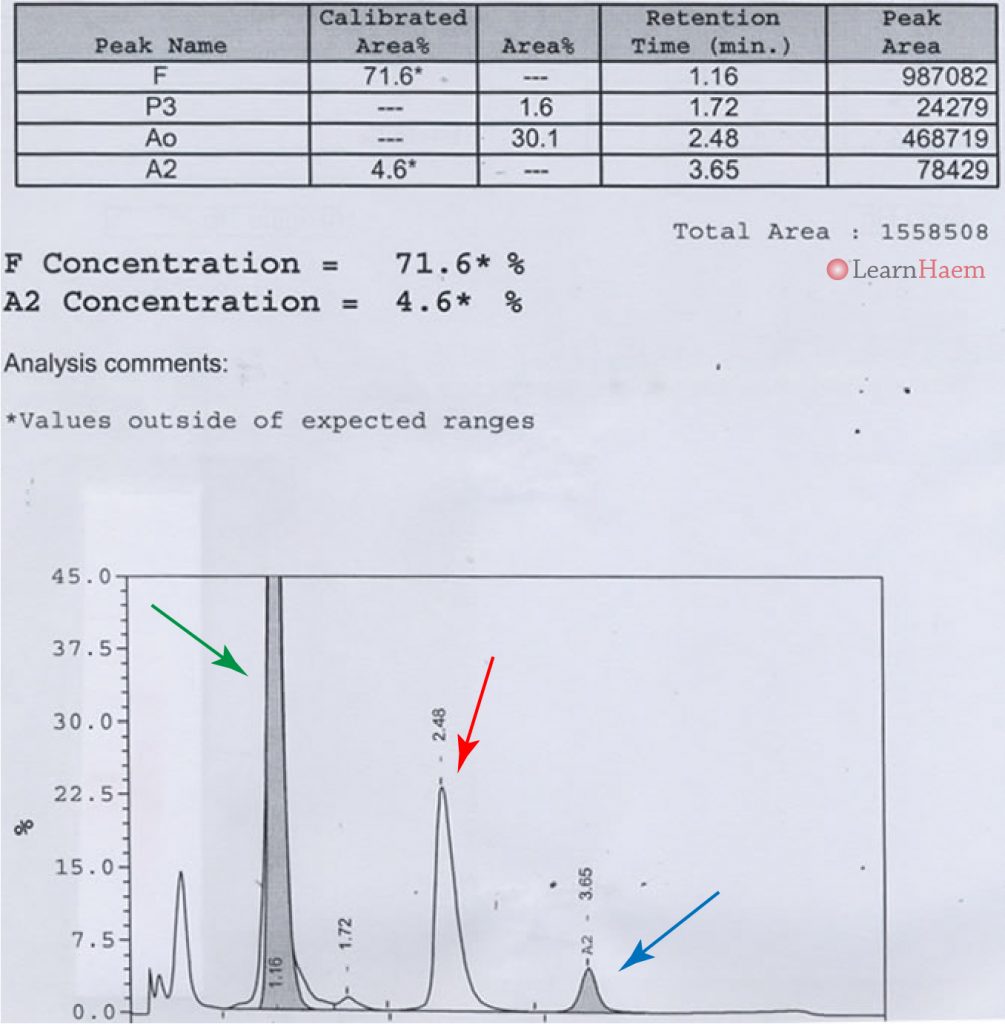
HPLC from a patient with ß thalassaemia intermedia. The majority (~70%) of the haemoglobin is haemoglobin F (green arrow). The main differential for such a high HbF is hereditary persistence of fetal haemoglobin (HPFH). However, HPFH is a benign condition not associated with anaemia, which makes the diagnosis unlikely here. There is normal haemoglobin A (red arrow), as well as a slightly increased fraction of haemoglobin A2 (4.6%, blue arrow). The low fraction of HbA2 makes Hb E unlikely, as it is usually present in quantities of ~30%.
The main differentials for such an appearance on HPLC are ß thalassaemia intermedia, or ß thalassaemia major post-transfusion (in native ß major, no normal haemoglobin A is present).
Other resources:
- PHE Family Origin Questionnaire
- PHE Sickle Cell and Thalassaemia Screening Programme (2019)
- BCSH Guideline: Significant Haemoglobinopathies: Guidelines for Screening and Diagnosis (2010)
- BCSH Guideline: Red blood cell specifications for patients with hemoglobinopathies: a systematic review and guideline (2020)
- RCOG Guideline: Management of ß Thalassaemia in Pregnancy (2014)
- TIF Guideline: Management of Non-Transfusion Dependent Thalassaemia (2017)
Leave A Comment