
The natural history of chronic myeloid leukaemia (CML) is to progress to accelerated and finally blast phases. The diagnosis is based on haematological and cytogenetic criteria, as well as clinical response to therapy. The treatment of CML in accelerated phase is more difficult.
Diagnostic Criteria (WHO 2016)
CML-AP is defined by the presence of ≥ 1 of the following haematological/cytogenetic criteria or provisional criteria concerning response to tyrosine kinase inhibitor (TKI) therapy
Haematological/cytogenetic criteria
- Persistent or increasing high white blood cell count (>10 x 109/L), unresponsive to therapy
- Persistent or increasing splenomegaly, unresponsive to therapy
- Persistent thrombocytosis (>1000 x 109/L), unresponsive to therapy
- Persistent thrombocytopenia (<100 x 109/L), unrelated to therapy
- ≥ 20% basophils in the peripheral blood
- 10-19% blasts in the peripheral blood and/or bone marrow
- Additional clonal chromosomal abnormalities in Philadelphia (Ph) chromosome-positive (Ph+) cells at
diagnosis, including so―called major route abnormalities (a second Ph chromosome, trisomy 8,
isochromosome 17q, trisomy 19), complex karyotype, and abnormalities of 3q26.2 - Any new clonal chromosomal abnormality in Ph+ cells that occurs during therapy
Provisional response to TKI criteria
- Haematological resistance (or failure to achieve a complete haematological response d) to the first TKI
- Any haematological, cytogenetic, or molecular indications of resistance to two sequential TKIs
- Occurrence of two or more mutations in the BCR-ABL1 fusion gene during TKI therapy


0 x
0 x
0 x
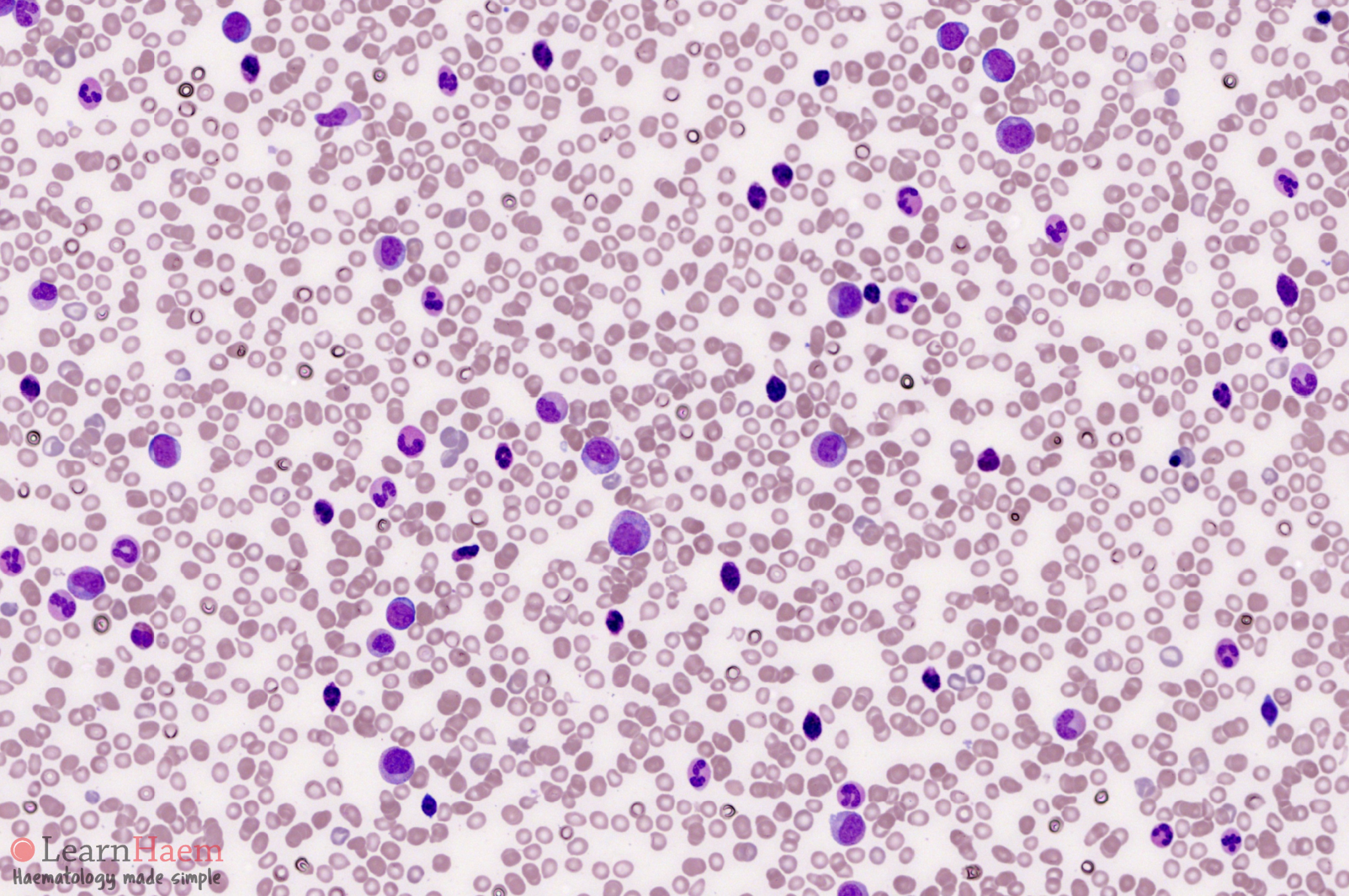
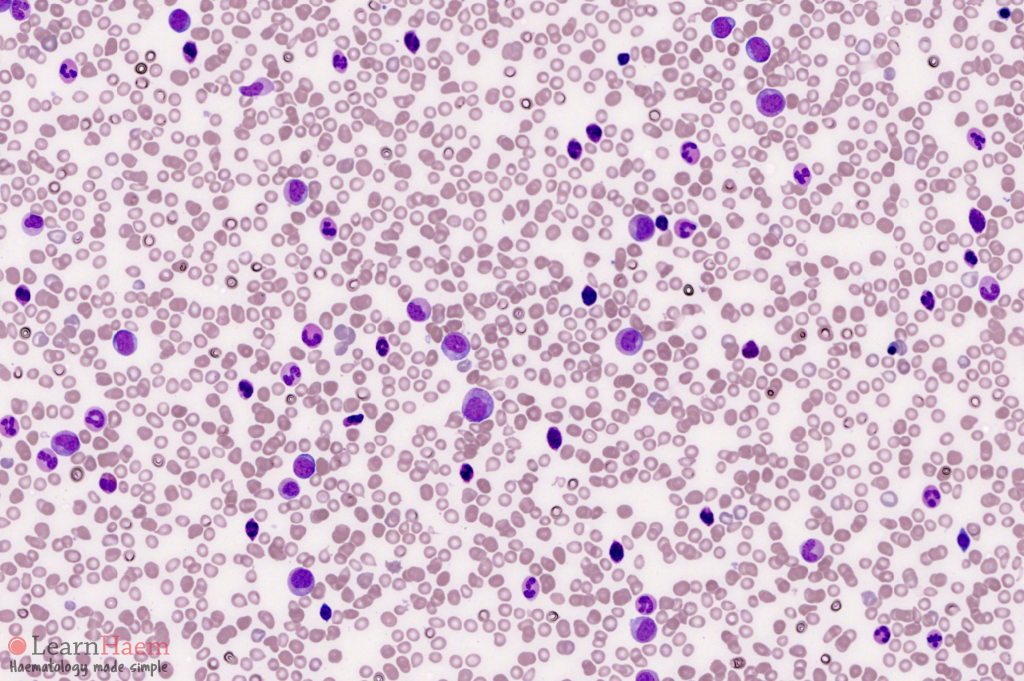
Blood Film Features:
- Overall features similar to CML in chronic phase
- Blast percentage 10-19%
- Basophilia > 20%
0 x
0 x
0 x
Bone Marrow Features:
- Overall features similar to CML in chronic phase
- Blast percentage 10-19%: access blast morphological lineage (Any presence of lymphoid blast is a red flag for impending progression to lymphoid blast crisis)
Leave A Comment